A grim warning from Israel: Vaccination blunts, but does not defeat Delta(science.org)
science.org
A grim warning from Israel: Vaccination blunts, but does not defeat Delta
https://www.science.org/news/2021/08/grim-warning-israel-vaccination-blunts-does-not-defeat-delta
101 comments
Agree 100%. A friend of mine shared the article this morning and I basically said the same. By itself the 60% is a meaningless number and says nothing about the vaccine efficacy.
> An embarrassing failure for science.org
Yes. Looking at the author's bio, you would expect a more nuanced comment and not this kind of fear mongering.
Meredith Wadman
Meredith joined Science as a staff writer in September 2016, after covering biomedical research and its politics from Washington, D.C., for 20 years. Her current beat includes biology research, policy, and sexual harassment . She has been a staff writer for Nature and a contributing writer at Fortune. She has also written op-eds for The Wall Street Journal, The New York Times and The Washington Post. Her first book, The Vaccine Race: Science, Politics and the Human Costs of Defeating Disease, was published by Viking (U.S./Canada) and Transworld (U.K.) in February 2017. Meredith earned her B.A. in Human Biology at Stanford University and began medical school at the University of British Columbia in her native Vancouver. She completed her medical degree as a Rhodes Scholar at the University of Oxford in the United Kingdom, and earned a master’s of science at the Columbia University Graduate School of Journalism.
> An embarrassing failure for science.org
Yes. Looking at the author's bio, you would expect a more nuanced comment and not this kind of fear mongering.
Meredith Wadman
Meredith joined Science as a staff writer in September 2016, after covering biomedical research and its politics from Washington, D.C., for 20 years. Her current beat includes biology research, policy, and sexual harassment . She has been a staff writer for Nature and a contributing writer at Fortune. She has also written op-eds for The Wall Street Journal, The New York Times and The Washington Post. Her first book, The Vaccine Race: Science, Politics and the Human Costs of Defeating Disease, was published by Viking (U.S./Canada) and Transworld (U.K.) in February 2017. Meredith earned her B.A. in Human Biology at Stanford University and began medical school at the University of British Columbia in her native Vancouver. She completed her medical degree as a Rhodes Scholar at the University of Oxford in the United Kingdom, and earned a master’s of science at the Columbia University Graduate School of Journalism.
The 60% is also not adjusted for age, see here for good explanations:
https://www.washingtonpost.com/outlook/2021/08/31/covid-isra...
https://www.covid-datascience.com/post/israeli-data-how-can-...
This is such an important point, I think it's worth including the key table here:
Vaccine effectiveness vs. severe disease for younger (<50yr) = 1 - 0.3/3.9 = 91.8%
Vaccine effectiveness vs. severe disease for older (>50yr) = 1- 13.6/91.9 = 85.2%
But if you combine the two, you get 67.5% !!!! which is the # people have been wrongly focused on.
https://www.washingtonpost.com/outlook/2021/08/31/covid-isra...
https://www.covid-datascience.com/post/israeli-data-how-can-...
This is such an important point, I think it's worth including the key table here:
Vaccine effectiveness vs. severe disease for younger (<50yr) = 1 - 0.3/3.9 = 91.8%
Vaccine effectiveness vs. severe disease for older (>50yr) = 1- 13.6/91.9 = 85.2%
But if you combine the two, you get 67.5% !!!! which is the # people have been wrongly focused on.
I think it must be something about the incentives of publishing.
[deleted]
You make a good point about the conditional probabilities.
The article also said "most". There is some relatively good data from Israel, but, still, in practice most doesn't just mean > 50% but is essentially wildly undefined. So apparently the author(s) of the article like to write with emotional adjectives instead of important numerical data.
The authors were trained in belle lettre (maybe art as in communication, interpretation of human experience, emotion or VEFEEE -- vicarious escapist fantasy emotional experience entertainment) or just like to grab people by the heart, the gut, below the belt to get eyeballs for ad revenue? Whatever, when they got to most I quit reading.
The article also said "most". There is some relatively good data from Israel, but, still, in practice most doesn't just mean > 50% but is essentially wildly undefined. So apparently the author(s) of the article like to write with emotional adjectives instead of important numerical data.
The authors were trained in belle lettre (maybe art as in communication, interpretation of human experience, emotion or VEFEEE -- vicarious escapist fantasy emotional experience entertainment) or just like to grab people by the heart, the gut, below the belt to get eyeballs for ad revenue? Whatever, when they got to most I quit reading.
> Trivially, and to make the point, if 100% of people are vaccinated, then 100% of hospitalizations will be among the vaccinated
I mean, that's still scary, people were hoping for exactly 0% of covid-related hospitalization if you're vaccinated
I mean, that's still scary, people were hoping for exactly 0% of covid-related hospitalization if you're vaccinated
I can't argue about what general public thought; but I think the epidemiological consensus even before we had experience with these vaccines is that vaccine effectiveness wouldn't be 100%--based on our experience with other vaccines. Instead, we rely on population effects to do the work.
If susceptibility to infection is above some point in the general population, then infections become a self-sustaining cascade through social networks (of course, the composition and structure of that network also matter--I'm simplifying). But if you can push susceptibility lower enough, the infections will not cause self-sustaining cascades.
This is, btw, why I consider anti-vaxxers (in the before times) as free-loaders who relied on those around them being vaccinated to protect them.
If susceptibility to infection is above some point in the general population, then infections become a self-sustaining cascade through social networks (of course, the composition and structure of that network also matter--I'm simplifying). But if you can push susceptibility lower enough, the infections will not cause self-sustaining cascades.
This is, btw, why I consider anti-vaxxers (in the before times) as free-loaders who relied on those around them being vaccinated to protect them.
Anti-vaxxers won't be effectively protected long term by those around them being vaccinated. The Delta variant is sufficiently contagious that there will be no significant herd immunity effect. All of us can expect to get exposed eventually.
https://www.businessinsider.com/delta-variant-made-herd-immu...
https://www.businessinsider.com/delta-variant-made-herd-immu...
I think this is why I didn't include the covid-anti-vaxxers in that mix; they're more like covid fatalists. Absent a vaccine, covid-fatalism--the idea that you will get it eventually--is not insane. Lots of simulations show you can flatten the curve with various measures, but the area under the curve ends up being the same in the long run; or at least that's my lay person understanding of it. Not getting everyone sick at once keeps everything getting overwhelmed at once ... but long sustained restrictions have costs too.
But all that logic is really thrown out the window with widespread availability of effective vaccines.
But all that logic is really thrown out the window with widespread availability of effective vaccines.
I'd be more concerned that 100% of people are vaccinated and that's still not enough to stop transmission.
indeed, strange article.
It is however quite possible at this point, that the effectiveness against symptomatic infection wears off to nearly zero after 5-6 months.
This seems to be the cause with both mRNA and sinopharm's inactivated virus vaccine as well.
It is however quite possible at this point, that the effectiveness against symptomatic infection wears off to nearly zero after 5-6 months.
This seems to be the cause with both mRNA and sinopharm's inactivated virus vaccine as well.
I think the science always knew this, but they mislead the population because being vaccinated is still better than not. The whole vaccination thing is a white lie.
We have never eradicated the flu, it mutates too fast. Same is true with Covid-19. The medical establishment has always known this, yet they spread propaganda because, again, being vaccinated is safer. The numbers about 99% effective were a lie, they knew it would mutate and that would see a drastic drop.
I would argue this is a dangerous game they are playing with public trust.
We have never eradicated the flu, it mutates too fast. Same is true with Covid-19. The medical establishment has always known this, yet they spread propaganda because, again, being vaccinated is safer. The numbers about 99% effective were a lie, they knew it would mutate and that would see a drastic drop.
I would argue this is a dangerous game they are playing with public trust.
Could you provide a source for your 99%, given you're accusing others of lying?
The numbers I have are ~96% for the Pfizer, and ~94% for Moderna.
I explain this in another comment below, but even against Delta, the efficacy is actually quite high, even in the Israeli data:
Vaccine effectiveness vs. severe disease for younger (<50yr) = 1 - 0.3/3.9 = 91.8%
Vaccine effectiveness vs. severe disease for older (>50yr) = 1- 13.6/91.9 = 85.2%
The combined number suffers from Simpson's paradox, please read more:
https://www.covid-datascience.com/post/israeli-data-how-can-...
& please stop spreading misinformation. 96-94% to 85-91% is against a new variant is hardly a drastic drop. The vaccine is saving millions of lives globally.
The numbers I have are ~96% for the Pfizer, and ~94% for Moderna.
I explain this in another comment below, but even against Delta, the efficacy is actually quite high, even in the Israeli data:
Vaccine effectiveness vs. severe disease for younger (<50yr) = 1 - 0.3/3.9 = 91.8%
Vaccine effectiveness vs. severe disease for older (>50yr) = 1- 13.6/91.9 = 85.2%
The combined number suffers from Simpson's paradox, please read more:
https://www.covid-datascience.com/post/israeli-data-how-can-...
& please stop spreading misinformation. 96-94% to 85-91% is against a new variant is hardly a drastic drop. The vaccine is saving millions of lives globally.
When we make accusations like this, its becoming to actually point to specific examples where specific individuals or organizations have done this. For example, this doesn't accord with my recollection, by my recollection is skewed in various ways.
In my opinion science should be about Truth, the rest should be left to people and their leaders. Truth being central to the process of science is what makes science unique and allows for societies to accumulate knowledge.
It's no game.The vaccine was extremely effective. After a year, a new vaccine will be needed for the new strains. Just like the flu vaccines.
p(i|v) = ( p(v|i) * p(i) ) / p(v)
p(v|i) = 0.6
p(v) = 0.6
p(i) = ?; but it's high (record case counts)
p(i|v) = p(i); high
That is why considering age is important and why interacting variables make it so easy for statistics to mislead when talking to people who are less verse or aren’t aware of the topic being studied.
About 78% of those above 12 are vaccinated in Israel, and the rate is even higher for those more susceptible to the virus.
Without quantifying those factors, it’s going to lead to a garbage in garbage out assessment.
About 78% of those above 12 are vaccinated in Israel, and the rate is even higher for those more susceptible to the virus.
Without quantifying those factors, it’s going to lead to a garbage in garbage out assessment.
No, because you assume that a 10 year old has an equal probability of being hospitalised as a 90 year old (for example).
Israel has a low overall vaccination rate because they have a very young population.
If you restrict the sample to just >50 year olds (majority of hospitalisations), then both statistics look very different.
Israel has a low overall vaccination rate because they have a very young population.
If you restrict the sample to just >50 year olds (majority of hospitalisations), then both statistics look very different.
Based on CDC data a 90 year old has at least 30× the risk of hospitalization compared to a 10 year old.
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burd...
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burd...
Well, the article says 78% of people 12 yo and older are vaccinated in Israel. Not sure what percent if you drop it to include everyone.
87% of those who were hospitalized were 60 or older (which doesn't match the general population). I imagine that vaccination rates are much much higher than 60% among those over 60. In the US its around 80%. But also, hospitalizations are much more likely the older you get. Moreover (and this was the point of the paper the article was discussing), the effectiveness of the vaccine may dwindle with time, and the 60+ crowd were among the first to get vaccinated.
So, no, I don't think you can do so simple a calculation and conclude that.
Instead of back of the envelope estimates, I think I'd just point to this study: https://www.nejm.org/doi/full/10.1056/NEJMoa2108891
Abstract:
Background
The B.1.617.2 (delta) variant of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (Covid-19), has contributed to a surge in cases in India and has now been detected across the globe, including a notable increase in cases in the United Kingdom. The effectiveness of the BNT162b2 and ChAdOx1 nCoV-19 vaccines against this variant has been unclear. Methods
We used a test-negative case–control design to estimate the effectiveness of vaccination against symptomatic disease caused by the delta variant or the predominant strain (B.1.1.7, or alpha variant) over the period that the delta variant began circulating. Variants were identified with the use of sequencing and on the basis of the spike (S) gene status. Data on all symptomatic sequenced cases of Covid-19 in England were used to estimate the proportion of cases with either variant according to the patients’ vaccination status. Results
Effectiveness after one dose of vaccine (BNT162b2 or ChAdOx1 nCoV-19) was notably lower among persons with the delta variant (30.7%; 95% confidence interval [CI], 25.2 to 35.7) than among those with the alpha variant (48.7%; 95% CI, 45.5 to 51.7); the results were similar for both vaccines. With the BNT162b2 vaccine, the effectiveness of two doses was 93.7% (95% CI, 91.6 to 95.3) among persons with the alpha variant and 88.0% (95% CI, 85.3 to 90.1) among those with the delta variant. With the ChAdOx1 nCoV-19 vaccine, the effectiveness of two doses was 74.5% (95% CI, 68.4 to 79.4) among persons with the alpha variant and 67.0% (95% CI, 61.3 to 71.8) among those with the delta variant. Conclusions
Only modest differences in vaccine effectiveness were noted with the delta variant as compared with the alpha variant after the receipt of two vaccine doses. Absolute differences in vaccine effectiveness were more marked after the receipt of the first dose. This finding would support efforts to maximize vaccine uptake with two doses among vulnerable populations. (Funded by Public Health England.)
87% of those who were hospitalized were 60 or older (which doesn't match the general population). I imagine that vaccination rates are much much higher than 60% among those over 60. In the US its around 80%. But also, hospitalizations are much more likely the older you get. Moreover (and this was the point of the paper the article was discussing), the effectiveness of the vaccine may dwindle with time, and the 60+ crowd were among the first to get vaccinated.
So, no, I don't think you can do so simple a calculation and conclude that.
Instead of back of the envelope estimates, I think I'd just point to this study: https://www.nejm.org/doi/full/10.1056/NEJMoa2108891
Abstract:
Background
The B.1.617.2 (delta) variant of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (Covid-19), has contributed to a surge in cases in India and has now been detected across the globe, including a notable increase in cases in the United Kingdom. The effectiveness of the BNT162b2 and ChAdOx1 nCoV-19 vaccines against this variant has been unclear. Methods
We used a test-negative case–control design to estimate the effectiveness of vaccination against symptomatic disease caused by the delta variant or the predominant strain (B.1.1.7, or alpha variant) over the period that the delta variant began circulating. Variants were identified with the use of sequencing and on the basis of the spike (S) gene status. Data on all symptomatic sequenced cases of Covid-19 in England were used to estimate the proportion of cases with either variant according to the patients’ vaccination status. Results
Effectiveness after one dose of vaccine (BNT162b2 or ChAdOx1 nCoV-19) was notably lower among persons with the delta variant (30.7%; 95% confidence interval [CI], 25.2 to 35.7) than among those with the alpha variant (48.7%; 95% CI, 45.5 to 51.7); the results were similar for both vaccines. With the BNT162b2 vaccine, the effectiveness of two doses was 93.7% (95% CI, 91.6 to 95.3) among persons with the alpha variant and 88.0% (95% CI, 85.3 to 90.1) among those with the delta variant. With the ChAdOx1 nCoV-19 vaccine, the effectiveness of two doses was 74.5% (95% CI, 68.4 to 79.4) among persons with the alpha variant and 67.0% (95% CI, 61.3 to 71.8) among those with the delta variant. Conclusions
Only modest differences in vaccine effectiveness were noted with the delta variant as compared with the alpha variant after the receipt of two vaccine doses. Absolute differences in vaccine effectiveness were more marked after the receipt of the first dose. This finding would support efforts to maximize vaccine uptake with two doses among vulnerable populations. (Funded by Public Health England.)
[deleted]
Yeah, I got the overall vaccination rate from Google (60%), but as you say, the differences in age groups matter.
[deleted]
Exactly the same as “x% of automobile deaths were not using the safety belt”… What happens when everybody uses it?
[deleted]
Fair point.
The calculations running over hospitalization numbers tend to show that vaccines are ~85% effective in preventing hospitalization, usually by showing the reduction in N/100k cases.
That is what I've seen as well.
Base Rate Fallacy on science.org ?
https://en.wikipedia.org/wiki/Base_rate_fallacy
https://en.wikipedia.org/wiki/Base_rate_fallacy
That page explains the fallacy poorly. Like a lot of Wikipedia articles on technical topics, it gives an explanation that only makes sense to people who already know the concept (or at least I assume it does). For the rest of us, maybe someone could provide a clearer explanation?
I think this is the same as my earlier comment here https://news.ycombinator.com/item?id=28273947
Quote:
---
This number is meaningless without also knowing what percentage of the people are vaccinated. Compare:
"80% of the people in hospital have $foo, and 80% of the general population has $foo" - $foo has no bearing at all on hospitalisation.
"80% of the people in hospital have $spon, and 5% of the general population has $spon" - $spon is clearly linked to the majority of hospitalisations.
"45% of the people in hospital have $bar, and 5% of the general population has $bar" - $bar is linked to higher rates of hospitalisation, _despite_ not being the majority of hospitalisations.
Spoiler: for some age groups in the UK now, "being unvaccinated" is much like $bar.
---
I would add now:
"not $bar -" i.e. "being vaccinated" could make up "55% of the people in hospital" (or more) despite reducing the odds of it.
and "not wearing seatbelt" -> "in hospital after a car crash" is probably like the $spon case.
Those examples above of course come with the caveat "all other things being equal" which isn't the case if, e.g. that others have raised, the age breakdown of the whole population vs hospitalisation is different. That's why there are graphs of "over 50s, vaccinated vs. hospitalised" as a catogory.
Quote:
---
This number is meaningless without also knowing what percentage of the people are vaccinated. Compare:
"80% of the people in hospital have $foo, and 80% of the general population has $foo" - $foo has no bearing at all on hospitalisation.
"80% of the people in hospital have $spon, and 5% of the general population has $spon" - $spon is clearly linked to the majority of hospitalisations.
"45% of the people in hospital have $bar, and 5% of the general population has $bar" - $bar is linked to higher rates of hospitalisation, _despite_ not being the majority of hospitalisations.
Spoiler: for some age groups in the UK now, "being unvaccinated" is much like $bar.
---
I would add now:
"not $bar -" i.e. "being vaccinated" could make up "55% of the people in hospital" (or more) despite reducing the odds of it.
and "not wearing seatbelt" -> "in hospital after a car crash" is probably like the $spon case.
Those examples above of course come with the caveat "all other things being equal" which isn't the case if, e.g. that others have raised, the age breakdown of the whole population vs hospitalisation is different. That's why there are graphs of "over 50s, vaccinated vs. hospitalised" as a catogory.
What is not being said is some people are on the brink of death anyways and being vaccinated will not stop that trajectory(dying). The older you are the weaker your immune system is.
A 97 year not vaccinated would most likely die after getting covid, either from the virus itself or an infection that happens after the body is weakened by the virus. The same fully vaccinated person may or may not die, if they do die its going to happen anyways but will be listed as a hospitalization/death from covid.
A few other things about Israels vaccine program.
- They started early(12/20) so I imagine alot of the populace is starting to run into vaccines that are less effective than if they were administered late Spring like US/UK and Europe.
- I don't know what the obesity levels are like in that country but the CDC says there is a strong correlation between being obese and covid severity with a person.
- Of the hospitalizations mentioned there is a strong indication of age being a cause for more severe illness:
>Of the 514, 59% were fully vaccinated. Of the vaccinated, 87% were 60 or older
A few other things about Israels vaccine program.
- They started early(12/20) so I imagine alot of the populace is starting to run into vaccines that are less effective than if they were administered late Spring like US/UK and Europe.
- I don't know what the obesity levels are like in that country but the CDC says there is a strong correlation between being obese and covid severity with a person.
- Of the hospitalizations mentioned there is a strong indication of age being a cause for more severe illness:
>Of the 514, 59% were fully vaccinated. Of the vaccinated, 87% were 60 or older
That's reasonably accurate but it's nothing new. The other endemic "common cold" coronaviruses already had a high fatality rate for frail elderly patients.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2095096/
There is a strong correlation between national obesity rates and COVID-19 death rates.
https://www.bmj.com/content/372/bmj.n623
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2095096/
There is a strong correlation between national obesity rates and COVID-19 death rates.
https://www.bmj.com/content/372/bmj.n623
Those people that are on the brink of death don't get the vaccine and probably skew the metric in the other way.
If you know the cancer patient has 2 weeks left you're not going to vaccinate him. If that same cancer patient dies with covid it'll be counted as an unvaxxed covid death
If you know the cancer patient has 2 weeks left you're not going to vaccinate him. If that same cancer patient dies with covid it'll be counted as an unvaxxed covid death
"Vaccine efficacy, effectiveness and protection"
https://www.who.int/news-room/feature-stories/detail/vaccine...
Vaccine efficacy is found in trials, vaccine effectiveness is dynamic depending WHEN you calculate it and its found after 'deployment in the field'
"A vaccine’s efficacy is measured in a controlled clinical trial and is based on how many people who got vaccinated developed the ‘outcome of interest’ (usually disease) compared with how many people who got the placebo (dummy vaccine) developed the same outcome. Once the study is complete, the numbers of sick people in each group are compared, in order to calculate the relative risk of getting sick depending on whether or not the subjects received the vaccine. From this we get the efficacy – a measure of how much the vaccine lowered the risk of getting sick. If a vaccine has high efficacy, a lot fewer people in the group who received the vaccine got sick than the people in the group who received the placebo."
vs
"Vaccine effectiveness is a measure of how well vaccines work in the real world. Clinical trials include a wide range of people – a broad age range, both sexes, different ethnicities and those with known medical conditions – but they cannot be a perfect representation of the whole population. The efficacy seen in clinical trials applies to specific outcomes in a clinical trial . Effectiveness is measured by observing how well the vaccines work to protect communities as a whole. Effectiveness in the real world can differ from the efficacy measured in a trial, because we can’t predict exactly how effective vaccination will be for a much bigger and more variable population getting vaccinated in more real life conditions."
https://www.who.int/news-room/feature-stories/detail/vaccine...
Vaccine efficacy is found in trials, vaccine effectiveness is dynamic depending WHEN you calculate it and its found after 'deployment in the field'
"A vaccine’s efficacy is measured in a controlled clinical trial and is based on how many people who got vaccinated developed the ‘outcome of interest’ (usually disease) compared with how many people who got the placebo (dummy vaccine) developed the same outcome. Once the study is complete, the numbers of sick people in each group are compared, in order to calculate the relative risk of getting sick depending on whether or not the subjects received the vaccine. From this we get the efficacy – a measure of how much the vaccine lowered the risk of getting sick. If a vaccine has high efficacy, a lot fewer people in the group who received the vaccine got sick than the people in the group who received the placebo."
vs
"Vaccine effectiveness is a measure of how well vaccines work in the real world. Clinical trials include a wide range of people – a broad age range, both sexes, different ethnicities and those with known medical conditions – but they cannot be a perfect representation of the whole population. The efficacy seen in clinical trials applies to specific outcomes in a clinical trial . Effectiveness is measured by observing how well the vaccines work to protect communities as a whole. Effectiveness in the real world can differ from the efficacy measured in a trial, because we can’t predict exactly how effective vaccination will be for a much bigger and more variable population getting vaccinated in more real life conditions."
Thank you. This distinction is often forgotten and the terms used interchangeably in articles and debates
How is this grim? Case numbers are mostly irrelevant now. What really matters is the death rate. Very few vaccinated people die, and the death rate for unvaccinated children is also extremely low. All of us are likely to become a "case" at some point no matter what we do.
https://www.businessinsider.com/delta-variant-made-herd-immu...
https://www.businessinsider.com/delta-variant-made-herd-immu...
case numbers of course matter, because vaccines do not guarantee you will not end up with long covid, or many other consequences of a rough viral infection.
Countless millions will live with a permanent disability their entire life.
Countless millions will live with a permanent disability their entire life.
> Countless millions will live with a permanent disability their entire life.
Extraordinary claims require extraordinary evidence. I see no reason to believe this at all. Side effects from a viral infection, and specifically coronaviruses, lasting for months or even a year or two afterward in uncommon cases are well documented. To say that "countless millions will live with a permanent disability" with regard to a virus that has only even existed in humans for ~2 years now is completely unfounded, and over dramatic.
Extraordinary claims require extraordinary evidence. I see no reason to believe this at all. Side effects from a viral infection, and specifically coronaviruses, lasting for months or even a year or two afterward in uncommon cases are well documented. To say that "countless millions will live with a permanent disability" with regard to a virus that has only even existed in humans for ~2 years now is completely unfounded, and over dramatic.
[deleted]
The important thing is that the vaccines are having a large effect on Covid-related deaths. Despite the current number of reported cases in Israel being equal to (or even a bit over) the January peak, the number of deaths is much lower.
According to Google's numbers, their current 7-day average number of deaths is 23, while in January they had a 7-day average of about 65. And it looks like the deaths peaked in the past week.
https://www.google.com/search?q=israel+covid+cases&rlz=1C1CH...
For reference, the numbers in Florida (where vaccination rates are significantly lower) look a lot different. You have many more cases and more deaths than the January peak.
https://www.google.com/search?q=florida+covid+cases&rlz=1C1C...
According to Google's numbers, their current 7-day average number of deaths is 23, while in January they had a 7-day average of about 65. And it looks like the deaths peaked in the past week.
https://www.google.com/search?q=israel+covid+cases&rlz=1C1CH...
For reference, the numbers in Florida (where vaccination rates are significantly lower) look a lot different. You have many more cases and more deaths than the January peak.
https://www.google.com/search?q=florida+covid+cases&rlz=1C1C...
Vaccines are very effective at reducing the death rate but when making comparisons between countries or states we also have to adjust for population demographics. Florida has a median age of 42 whereas in Israel it's only 30. And more importantly Florida has 21% of the population over age 65 whereas in Israel it's only 12%. We know that age is a huge risk factor.
I keep hearing that Covid is never going away (see recent Atlantic article). How is it surprising when vaccines designed to prevent hospitalization don't prevent infection.
I imagine that it does make infection less likely, and make the likelihood of passing it on less likely too. I mean, most of the research on it says exactly that. But nothing is perfect.
I have heard similarly from various outlets that "we'll just have to learn to live with Covid-19, like we do with the flu and other viruses that we're unable to eradicate".
What I find curious is that SARS-CoV-1 (e.g. the original SARS circa 2003) seemed to eventually disappear overnight. It leaves me pondering two questions:
1. Did SARS-CoV-1 actually disappear or do we just not hear about it anymore?
2. What is different between SARS-CoV-1 and SARS-CoV-2 that makes us think the latter will persist indefinitely when the former seemed to disappear?
What I find curious is that SARS-CoV-1 (e.g. the original SARS circa 2003) seemed to eventually disappear overnight. It leaves me pondering two questions:
1. Did SARS-CoV-1 actually disappear or do we just not hear about it anymore?
2. What is different between SARS-CoV-1 and SARS-CoV-2 that makes us think the latter will persist indefinitely when the former seemed to disappear?
SARS-CoV was less contagious and had a higher fatality rate, so it burned out quickly. There's no reliable evidence that it's still circulating in humans.
SARS-CoV-2 is more contagious and less fatal so it has already spread worldwide. It also has multiple animal reservoirs so even if there was some way to simultaneously eliminate the virus from every human (there isn't), we would just catch it again from dogs or deer or something and the pandemic would restart.
SARS-CoV-2 is more contagious and less fatal so it has already spread worldwide. It also has multiple animal reservoirs so even if there was some way to simultaneously eliminate the virus from every human (there isn't), we would just catch it again from dogs or deer or something and the pandemic would restart.
There were only ever 8000 confirmed cases of SARS-CoV-1. It was able to be contained. Wikipedia mentions that quarantines were very effective because it wasn't often asymptomatically contagious.
https://en.wikipedia.org/wiki/Severe_acute_respiratory_syndr...
https://en.wikipedia.org/wiki/Severe_acute_respiratory_syndr...
Covid is the next Afghanistan.
Flu was the perfect crisis hiding right under our noses.
Variants have been circulating throughout the population causing a high number of deaths for all of modern history. Now that we’ve encountered a somewhat more deadly and contagious version than normal and the “danger” of this version has been super hyped, we’re quite sensitive to all flu related news, all flu variants, all flu deaths, etc. Confirmation bias at work. We’re now noticing something that was there all along: people die from the flu.
Even if actual flu related deaths reverted to a pre-2020 level, I guarantee it would still be news. People will still be wearing masks, state/local governments will be enforcing mandates, etc.
Couple the above with the fact that a group of bureaucrats have managed to seize an almost dictatorial amount of “emergency” powers, you can bet this isn’t going away anytime soon.
Variants have been circulating throughout the population causing a high number of deaths for all of modern history. Now that we’ve encountered a somewhat more deadly and contagious version than normal and the “danger” of this version has been super hyped, we’re quite sensitive to all flu related news, all flu variants, all flu deaths, etc. Confirmation bias at work. We’re now noticing something that was there all along: people die from the flu.
Even if actual flu related deaths reverted to a pre-2020 level, I guarantee it would still be news. People will still be wearing masks, state/local governments will be enforcing mandates, etc.
Couple the above with the fact that a group of bureaucrats have managed to seize an almost dictatorial amount of “emergency” powers, you can bet this isn’t going away anytime soon.
Even if actual flu related deaths reverted to a pre-2020 level, I guarantee it would still be news. People will still be wearing masks, state/local governments will be enforcing mandates, etc.
They were in pre-2020 for bad flu pandemics:
https://en.wikipedia.org/wiki/2009_swine_flu_pandemic_in_Mex...
They were in pre-2020 for bad flu pandemics:
https://en.wikipedia.org/wiki/2009_swine_flu_pandemic_in_Mex...
{kind=link}
You're aware the coronavirus isn't the flu, right? It's a totally different type of virus, completely unrelated to influenza.
> somewhat more deadly
A magnitude more deadly. Flu's death rate is ~.1%, Covid's is about 2-3%.
A magnitude more deadly. Flu's death rate is ~.1%, Covid's is about 2-3%.
> Covid's is about 2-3%.
0.7% in Israel. Much much less if you exclude terminal cancer, obesity and immunosuppressed transplant recipients.
0.7% in Israel. Much much less if you exclude terminal cancer, obesity and immunosuppressed transplant recipients.
Right. So, an overwhelming majority of the people who “died from COVID” would have likely passed away in the near future from something unrelated. They just were unfortunate enough to catch COVID in their already incredibly fragile and deteriorating state and end up with COVID listed as their cause of death.
If a person with cancer is hit by a bus, their death is not and should not be attributed to cancer. Likewise, if someone with a critical illness is robbed of their last few months by COVID, then it is correct to attribute their death to COVID.
The logic of "they were going to die anyways" means we might as well change every cause of death to "old age" or "natural causes", because if nothing else gets us, that's how we will all eventually die. But, of course, that would be stupid, and it would make death statistics meaningless - which is why we don't do it for COVID deaths.
The logic of "they were going to die anyways" means we might as well change every cause of death to "old age" or "natural causes", because if nothing else gets us, that's how we will all eventually die. But, of course, that would be stupid, and it would make death statistics meaningless - which is why we don't do it for COVID deaths.
> in their already incredibly fragile and deteriorating state
This state is called "dying". Dying people in ECU will develop pneumonia no matter what. If it would not be COVID, it would be their own gum bacteria.
This state is called "dying". Dying people in ECU will develop pneumonia no matter what. If it would not be COVID, it would be their own gum bacteria.
Remember that a third of the US is considered obese[1] and 10.5% of the population is diabetic[2], another common risk factor for covid.
You probably know a lot of people are in those groups.
[1] https://en.wikipedia.org/wiki/List_of_countries_by_obesity_r...
[2] https://www.cdc.gov/diabetes/pdfs/data/statistics/national-d...
You probably know a lot of people are in those groups.
[1] https://en.wikipedia.org/wiki/List_of_countries_by_obesity_r...
[2] https://www.cdc.gov/diabetes/pdfs/data/statistics/national-d...
That is misinformation. The CDC estimates COVID-19 death rate to be 0.6%. And vaccination cuts that rate close to 0.
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burd...
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burd...
Vaccination is moot as a point.
And even then... ok... COVID is only FIVE times more deadly, not 10.
It's not slightly more.
And even then... ok... COVID is only FIVE times more deadly, not 10.
It's not slightly more.
That is an insane, alarmist claim if I ever saw one. The death rate is absolutely not 2-3%.
What percentage of the population do think has been infected?
What percentage of the population do think has been infected?
Of cases reported, 2% have died. If you want to go with CDC estimates, it's about .6%, still 5X the flu. If you include all excess death's it's about .7-8%.
Pick your number but COVID <> The Flu.
I can't believe almost a million people have died and people still shrug it off as just the flu.
Pick your number but COVID <> The Flu.
I can't believe almost a million people have died and people still shrug it off as just the flu.
To be fair to GP, during the first few months of the pandemic - early to mid 2020 - this was the rate that was used in all publications. Though the rate might currently be known to be lower (or higher for all I know) this is the rate that I remember.
I remember earlier in the year talk of a Delta variant booster, but I haven't seen anything recently. Anyone have details?
Edit: looks like its in development. https://www.npr.org/2021/07/09/1014744345/pfizer-is-pursuing...
Edit: looks like its in development. https://www.npr.org/2021/07/09/1014744345/pfizer-is-pursuing...
I got the impression it was just another dose of the same vaccine(s) already available rather than a new thing.
I heard something about tests on vaccine combinations (i.e. different types of vaccine for your 1st & 2nd dose) a while back though but I can't remember the details, does anyone know what happened with that?
I heard something about tests on vaccine combinations (i.e. different types of vaccine for your 1st & 2nd dose) a while back though but I can't remember the details, does anyone know what happened with that?
At this point it is widely recognized that viral evolution is undermining the effectiveness of the current vaccines at preventing infection (~91% to ~66%) [1] and symptomatic illness (~95% to ~65%) [2].
Still, the benefits of vaccination remain significant - vaccines are helping prevent severe outcomes like hospitalization and death for many people.
Researching formulations that are more robust to viral resistance is already becoming a top priority. Diversifying viral elimination strategies at the population level will also be critical. Mandatory nonpharmaceutical interventions such as lock-downs and masking may help slow the spread of the virus, but at this point those measures will not stop the spread, because SARS-CoV-2 is highly contagious and primarily transmitted through the air (as acknowledged by the WHO and CDC) [3].
[1] Effectiveness of COVID-19 Vaccines in Preventing SARS-CoV-2 Infection Among Frontline Workers Before and During B.1.617.2 (Delta) Variant Predominance — Eight U.S. Locations, December 2020–August 2021 https://www.cdc.gov/mmwr/volumes/70/wr/mm7034e4.htm
[2] Resurgence of SARS-CoV-2 Infection in a Highly Vaccinated Health System Workforce https://www.nejm.org/doi/full/10.1056/NEJMc2112981
[3] Airborne transmission of respiratory viruses https://www.science.org/lookup/doi/10.1126/science.abd9149
Still, the benefits of vaccination remain significant - vaccines are helping prevent severe outcomes like hospitalization and death for many people.
Researching formulations that are more robust to viral resistance is already becoming a top priority. Diversifying viral elimination strategies at the population level will also be critical. Mandatory nonpharmaceutical interventions such as lock-downs and masking may help slow the spread of the virus, but at this point those measures will not stop the spread, because SARS-CoV-2 is highly contagious and primarily transmitted through the air (as acknowledged by the WHO and CDC) [3].
[1] Effectiveness of COVID-19 Vaccines in Preventing SARS-CoV-2 Infection Among Frontline Workers Before and During B.1.617.2 (Delta) Variant Predominance — Eight U.S. Locations, December 2020–August 2021 https://www.cdc.gov/mmwr/volumes/70/wr/mm7034e4.htm
[2] Resurgence of SARS-CoV-2 Infection in a Highly Vaccinated Health System Workforce https://www.nejm.org/doi/full/10.1056/NEJMc2112981
[3] Airborne transmission of respiratory viruses https://www.science.org/lookup/doi/10.1126/science.abd9149
> Researching formulations that are more robust to viral resistance is already becoming a top priority.
Are you aware of any good resources to help a lay person understand the basic concepts around this?
Are you aware of any good resources to help a lay person understand the basic concepts around this?
Some updates from Israel (based on Wednesday Sept 01 data)
"Some 11,246 new cases out of around 145,000 tests that were performed on Wednesday were diagnosed with the virus, the Health Ministry reported on Thursday evening, with 7.9% of those screened testing positive – the highest percentage since the start of the pandemic. Israel is in first place in the world in the number of daily cases per capita in the last seven days, according to international reports."
Source: https://www.jpost.com/health-and-wellness/coronavirus/israel...
To put it in perspective: 11246 cases in Israel, in proportion to the population, is roughly equivalent to 400K cases a day in US.
"Some 11,246 new cases out of around 145,000 tests that were performed on Wednesday were diagnosed with the virus, the Health Ministry reported on Thursday evening, with 7.9% of those screened testing positive – the highest percentage since the start of the pandemic. Israel is in first place in the world in the number of daily cases per capita in the last seven days, according to international reports."
Source: https://www.jpost.com/health-and-wellness/coronavirus/israel...
To put it in perspective: 11246 cases in Israel, in proportion to the population, is roughly equivalent to 400K cases a day in US.
Does anyone know what Israel is doing in terms of lockdowns, etc? Are they back to business as usual, or something else?
After two weeks in June mask mandate is back. Mass gatherings are limited. Certain fasciitis are available only to vaccinated.
Practically, nobody cares anymore. Compared to first lockdown, when streets were totally empty (a sight to behold), last half a year is business as usual.
Practically, nobody cares anymore. Compared to first lockdown, when streets were totally empty (a sight to behold), last half a year is business as usual.
I wonder if the solution is to look to structural reforms which are going to be more sustainable over the long term.
e.g. 4 day work week (2 days full shutdown) to reduce transmission by preventing people going into offices and businesses.
And mandatory training and financial support to all businesses to move online and remote.
e.g. 4 day work week (2 days full shutdown) to reduce transmission by preventing people going into offices and businesses.
And mandatory training and financial support to all businesses to move online and remote.
Israel indeed provides nice stats for Covid.
Especially where some of the population aren’t fully complying with suggested/requested measures. So we pretty much see the vaccination performance.
If it’s for health reasons (not leisure or traveling, PCR testing is free and there are many places available each day to test without scheduling.
Anyway, I was “fully vaccinated” on March 2020 iirc. I didn’t yet get the 3rd/booster shot. And I’m writing this being isolated with mild symptoms after testing positive for Covid. (Hoping symptoms will regress and I’ll be out within 10 days). I have no reliable assumption from where I got it and me and my oldest son are the only ones tested positive out of my close family and others we’ve been in touch with.
Especially where some of the population aren’t fully complying with suggested/requested measures. So we pretty much see the vaccination performance.
If it’s for health reasons (not leisure or traveling, PCR testing is free and there are many places available each day to test without scheduling.
Anyway, I was “fully vaccinated” on March 2020 iirc. I didn’t yet get the 3rd/booster shot. And I’m writing this being isolated with mild symptoms after testing positive for Covid. (Hoping symptoms will regress and I’ll be out within 10 days). I have no reliable assumption from where I got it and me and my oldest son are the only ones tested positive out of my close family and others we’ve been in touch with.
Hypothetical: Israelis were vaccinated very early compared to a lot of other countries. Maybe this is really just building the case for a booster? What's the correlation between hospitalization, severity, and time since last jab?
> What is clear is that “breakthrough” cases are not the rare events the term implies. As of 15 August, 514 Israelis were hospitalized with severe or critical COVID-19, a 31% increase from just 4 days earlier. Of the 514, 59% were fully vaccinated. Of the vaccinated, 87% were 60 or older. “There are so many breakthrough infections that they dominate and most of the hospitalized patients are actually vaccinated,”
If it's true that vaccines blunt the symptoms of infection, and that breakthrough cases still are as contagious as without vaccine (same viral load), then there could be more asymptomatic spreading by people who are not aware that they are contagious.
> and that breakthrough cases still are as contagious as without vaccine (same viral load),
I would _not_ assume that this is settled science.
This out today:
https://www.medrxiv.org/content/10.1101/2021.08.30.21262701v...
> These data indicate that vaccination shortens the duration of time of high transmission potential, minimizes symptom duration, and may restrict tissue dissemination.
I would _not_ assume that this is settled science.
This out today:
https://www.medrxiv.org/content/10.1101/2021.08.30.21262701v...
> These data indicate that vaccination shortens the duration of time of high transmission potential, minimizes symptom duration, and may restrict tissue dissemination.
Better article about the vaccine effectiveness
https://news.ycombinator.com/item?id=28221798
Israel went very heavily with Pfizer which ended up rather ineffective against Delta. With a more balanced mix they would have probably fared better.
> rather ineffective against Delta
I mean, this isn't true... less effective, sure. But it's not ineffective by any measure.
I mean, this isn't true... less effective, sure. But it's not ineffective by any measure.
https://www.medrxiv.org/content/10.1101/2021.08.06.21261707v...
If they had advertised 42% effectiveness rating when it was first launched they'd have probably gone back to the drawing board. (This is what Pfizer did recently with a second version that was aimed specifically at Delta but didn't fare any better than the first version.)
If they had advertised 42% effectiveness rating when it was first launched they'd have probably gone back to the drawing board. (This is what Pfizer did recently with a second version that was aimed specifically at Delta but didn't fare any better than the first version.)
Against the delta variant, the vaccine reduces transmission, significantly reduces severity, and significantly reduces risk of death: all extremely worthwhile goals.
Read https://www.kff.org/policy-watch/covid-19-vaccine-breakthrou...
Read https://www.kff.org/policy-watch/covid-19-vaccine-breakthrou...
78% vaccination, more than half of new are breakthrough, i.e. the vaccinated chances to get infected is more than 28% of that of unvaccinated. Similar numbers to MA https://www.bostonherald.com/2021/08/31/massachusetts-report... - 65% vaccination rate - out of the 1144 current average new daily infections the 500+ are breakthrough, ie. the chances are 40%. The data is probably skewed by the fact that vaccines smooth the symptoms and thus the breakthroughs are probably much more undercounted.
Vaccination is heavily correlated with age and age is heavily correlated with risk. So, you really need to do a more complex breakdown to understand what’s going on.
Aka if 90% of the 80+ year old population is vaccinated and 0% of the under 12 year old population is vaccinated then being unvaccinated starts to look like a good option. Except what you really want is to be young.
Aka if 90% of the 80+ year old population is vaccinated and 0% of the under 12 year old population is vaccinated then being unvaccinated starts to look like a good option. Except what you really want is to be young.
Tidbit: UK, being 0-17 and unvaccinated bears a smaller risk of covid related death than being >40 and vaccinated.
https://twitter.com/kerpen/status/1420401034376224775
https://twitter.com/kerpen/status/1420401034376224775
>Vaccination is heavily correlated with age
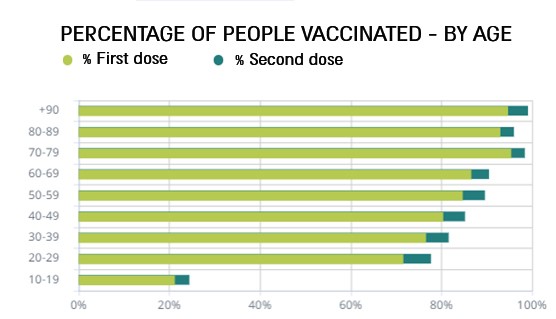
not really https://eu.boell.org/sites/default/files/2021-06/IL%2004.jpg
Except for teenagers as it was pointed out, though i usually didn't consider them because of being outliers wrt. history of vaccination. Well, lets consider them too. That is new cases by age http://cdn.statcdn.com/Infographic/images/normal/25295.jpeg
Let's look at opposites:
60-69 - 90% vaccination, 8% cases, 0.5M population
10-19 - 25% vaccination, 40% cases, 1.4M population.
I.e. almost 3x population, 5x cases with 25% vs 90% vaccination rate. Simple arithmetic - vaccinated chances to get infected are ~35% that of unvaccinated. Whatever way you slice and dice these numbers or the available numbers from other well vaccinated places like MA, UK, Singapore you always get in the 25%-40% ballpark.
not really https://eu.boell.org/sites/default/files/2021-06/IL%2004.jpg
{kind=link}
Except for teenagers as it was pointed out, though i usually didn't consider them because of being outliers wrt. history of vaccination. Well, lets consider them too. That is new cases by age http://cdn.statcdn.com/Infographic/images/normal/25295.jpeg
{kind=link}
Let's look at opposites:
60-69 - 90% vaccination, 8% cases, 0.5M population
10-19 - 25% vaccination, 40% cases, 1.4M population.
I.e. almost 3x population, 5x cases with 25% vs 90% vaccination rate. Simple arithmetic - vaccinated chances to get infected are ~35% that of unvaccinated. Whatever way you slice and dice these numbers or the available numbers from other well vaccinated places like MA, UK, Singapore you always get in the 25%-40% ballpark.
I think you misunderstood what I meant. As your first graph shows the elderly are more likely to be vaccinated than the young thus age correlates with vaccination rates.
However, youth is protection from serious complications or deaths. So if you look hospitalizations or deaths rather than positive tests for infections the graphs look very different. The Simpson’s paradox means your less likely to die after a COVID vaccination, but it’s easy to slice the data to make it look otherwise. https://en.wikipedia.org/wiki/Simpson%27s_paradox
However, youth is protection from serious complications or deaths. So if you look hospitalizations or deaths rather than positive tests for infections the graphs look very different. The Simpson’s paradox means your less likely to die after a COVID vaccination, but it’s easy to slice the data to make it look otherwise. https://en.wikipedia.org/wiki/Simpson%27s_paradox
i don't discuss the number of hospitalizations or deaths - that is currently established fact that the current vaccines decrease that (at least as the 1st order effect and leaving aside the possible 2nd order that infected vaccinated being undercounted and asymptomatic with higher chances may be walking around spreading) and there is not much point to discuss there. I discuss infection spread at which those vaccines fail, and thus various vaccine mandates policies and societal push for it are completely unfounded and based in hysteria and ideology.
Ok, that’s a different issue. We have crossed the threshold where most people are getting sick or vaccinated, with many getting both. People can test positive for infection without being particularly infectious. Just as the vaccinated are less likely to be hospitalized they are also vastly less contagious on average after infection.
That’s from two different effects the vaccinated and prior infected are both less sick and sick for a shorter periods. Which is why people talk about herd immunity. Of course the longer people go unvaccinated the more evolution is pushing COVID to become ever more infectious aka Delta as part of a long line of slightly worse variants.
But, again eventually almost everyone gets it or the vaccine so there is major pressure to get people vaccinated or just open up so the unvaccinated get sick.
That’s from two different effects the vaccinated and prior infected are both less sick and sick for a shorter periods. Which is why people talk about herd immunity. Of course the longer people go unvaccinated the more evolution is pushing COVID to become ever more infectious aka Delta as part of a long line of slightly worse variants.
But, again eventually almost everyone gets it or the vaccine so there is major pressure to get people vaccinated or just open up so the unvaccinated get sick.
[deleted]
Um, your graph shows that younger people are several times more likely to be unvaccinated than older people
I don't think the vaccine is creating a strong memory cell response.
The vaccine is probably just ramping up the immune system response for a few months. That alone would prevent death and since we don't really have anything else, it's still better than nothing.
The vaccine is probably just ramping up the immune system response for a few months. That alone would prevent death and since we don't really have anything else, it's still better than nothing.
Please don't post conjecture like this that has been categorically shown to be untrue. Vaccines are effective and have been shown to decrease infection and serious illness rates.
It's not conjecture[1] -- what is misinformation is the assertion "...has been categorically shown to be untrue". Citation?
I find that when people use "categorically" in an assertion (denial), then there's good reason for doubt.
1. https://www.forbes.com/sites/roberthart/2021/08/25/vaccine-p...
I find that when people use "categorically" in an assertion (denial), then there's good reason for doubt.
1. https://www.forbes.com/sites/roberthart/2021/08/25/vaccine-p...
You think you’re fighting misinformation, but GP could be right in terms of T cell response.
Vaccination has been shown to induce an immune response including T cells [1].
However, vaccination induces a slightly different immune response compared to natural infection [2][3] . These differences may account for variation in effectiveness between vaccine-induced and naturally acquired immunity.
[1] Rapid induction of antigen-specific CD4+ T cells is associated with coordinated humoral and cellular immune responses to SARS-CoV-2 mRNA vaccination https://www.cell.com/immunity/fulltext/S1074-7613(21)00308-3
[2] Antibodies elicited by mRNA-1273 vaccination bind more broadly to the receptor binding domain than do those from SARS-CoV-2 infection https://pubmed.ncbi.nlm.nih.gov/34103407/
[3] mRNA vaccination compared to infection elicits an IgG-predominant response with greater SARS-CoV-2 specificity and similar decrease in variant spike recognition https://www.medrxiv.org/content/medrxiv/early/2021/04/07/202...
However, vaccination induces a slightly different immune response compared to natural infection [2][3] . These differences may account for variation in effectiveness between vaccine-induced and naturally acquired immunity.
[1] Rapid induction of antigen-specific CD4+ T cells is associated with coordinated humoral and cellular immune responses to SARS-CoV-2 mRNA vaccination https://www.cell.com/immunity/fulltext/S1074-7613(21)00308-3
[2] Antibodies elicited by mRNA-1273 vaccination bind more broadly to the receptor binding domain than do those from SARS-CoV-2 infection https://pubmed.ncbi.nlm.nih.gov/34103407/
[3] mRNA vaccination compared to infection elicits an IgG-predominant response with greater SARS-CoV-2 specificity and similar decrease in variant spike recognition https://www.medrxiv.org/content/medrxiv/early/2021/04/07/202...
> differences may account for variation in effectiveness between vaccine-induced and naturally acquired immunity.
What's the variation you are referring to?
What's the variation you are referring to?
antibodies produced in a primary infection target a lot more than spike protein, in some pre-prints.
It's all preliminary data. However, the sinopharm vaccine, which is the whole virus, not just spike protein, seems to lose effectiveness after several months as well.
It's all preliminary data. However, the sinopharm vaccine, which is the whole virus, not just spike protein, seems to lose effectiveness after several months as well.
Then GP should have posted some evidence. It's lazy and hinders discourse to post a conjecture that can be quickly disproved with a quick search.
[deleted]
In fact, the scariest statistic it gives--that nearly 60% of serious hospitalizations are fully vaccinated) gives the p(vaccinated|infected), not p(infected|vaccinated).
Trivially, and to make the point, if 100% of people are vaccinated, then 100% of hospitalizations will be among the vaccinated--which tells you almost nothing about how likely it is to be hospitalized when vaccinated (beyond that its nonzero).
An embarrassing failure for science.org